腺癌
定義:腺腔形成、粘液産生、または肺胞上皮細胞マーカー(TTF-1, Napsin A)が陽性を示す悪性上皮性腫瘍
前浸潤性病変 1999年および2004年のWHO分類では,腺癌の亜型として浸潤のない腺癌をbrochioloalveolar carcinoma (BAC)と呼び,また腫瘍細胞が既存の肺胞壁に沿って増殖するパターンをBACパターン呼ぶように,BACを2種類の意味で用いている.また,必ずしも予後が良好ではない粘液産生性のBACも存在する.1999年および2004年のWHO分類では,前浸潤性病変として,異形成と上皮内癌,異型腺腫様過形成,びまん性特発性肺神経内分泌細胞過形成をあげているが,BACは浸潤のない腺癌であるのに前浸潤性病変に含まれていない.このような矛盾を解消するために,IASLC/ATS/ERS新分類では,BACという用語は用いず,かわりにlepidicパターンを用い,腺癌の前浸潤性病変として上皮内腺癌を加えた.
lepidicパターンとは?
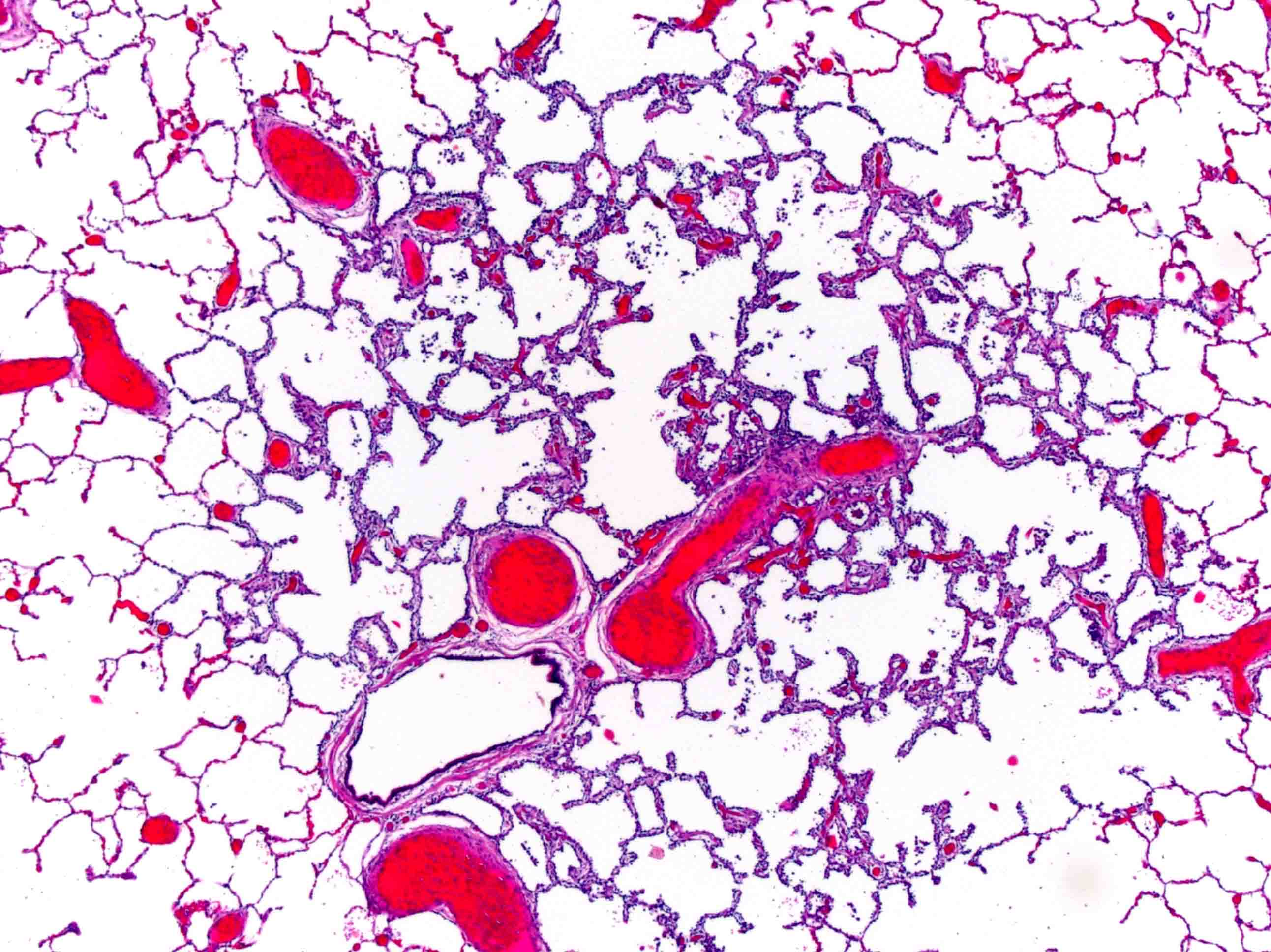
異型腺腫様過形成 Atypical adenomatous hyperplasia (AAH)
異型腺腫様過形成の大きさは,通常5mm以下であり,多発することもある.軽度から中等度の異型性を示すII型肺胞上皮細胞(あるいはクララ細胞)が肺胞壁(あるいは呼吸細気管支)に沿って増生するが,細胞と細胞の間に隙間がみられる.核内封入体がみられる.異型性が強く細胞密度が高い場合は,AAHと上皮内腺癌Adenocarcinoma in situ (AIS)の鑑別は難しい.
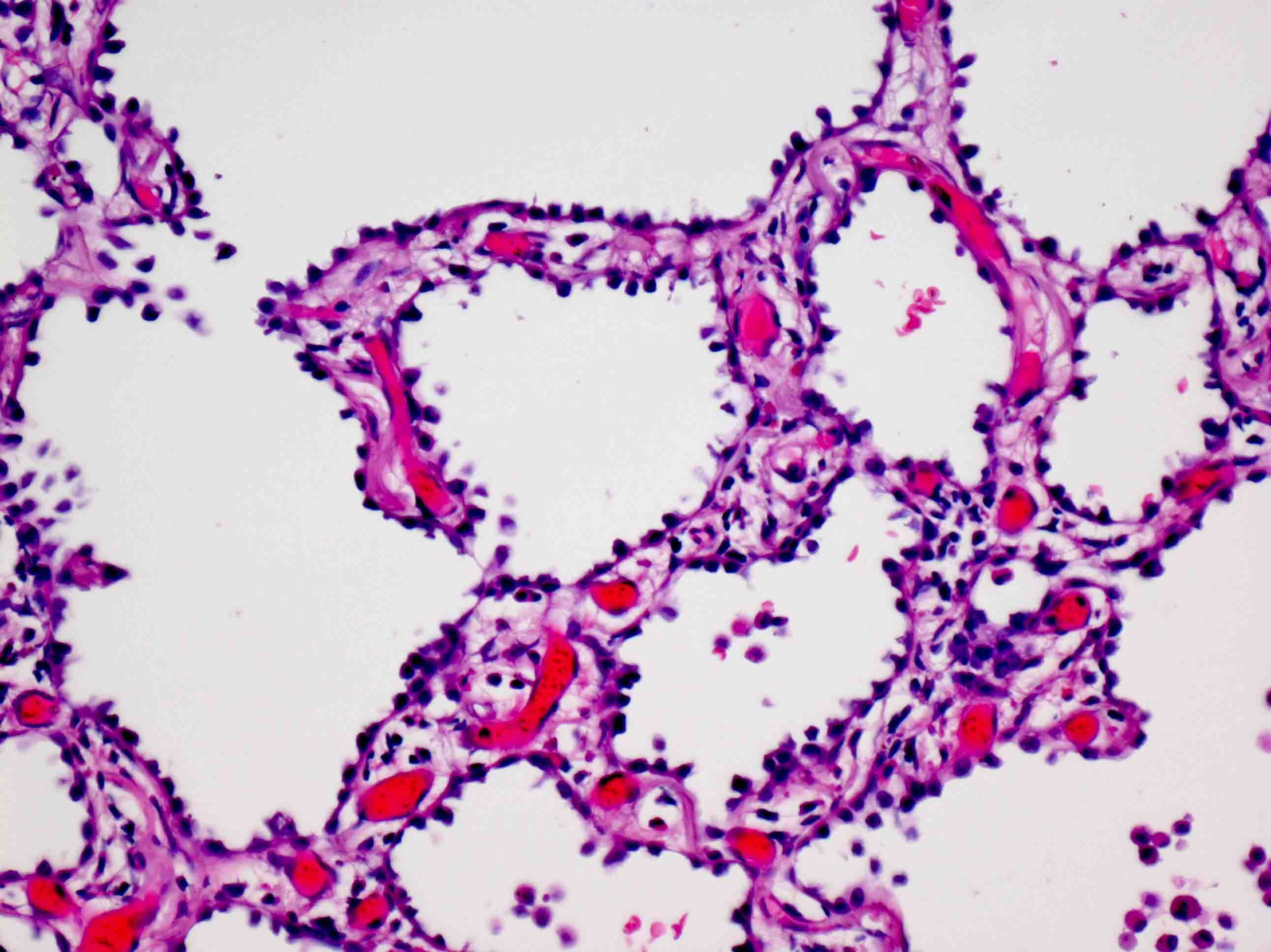
上皮内腺癌 Adenocarcinoma in situ (AIS)


従来のBACである.孤立性で,腫瘍径が3cm以下で,既存の肺胞壁に沿って腫瘍細胞が増殖し(lepidicパターン),間質,血管,胸膜への浸潤を認めないものをいう.乳頭型,微小乳頭型や肺胞腔内の腫瘍細胞はみられない.大半が粘液非産生性で,II型肺胞上皮あるいはClara細胞からなる.まれに,粘液産生性上皮内腺癌が存在する.これは,高円柱状細胞からなり,核は基底部に並び,細胞質に豊富な粘液を入れている.
腫瘍がlepidicパターンのみからなっても,腫瘍径が3cmを超える場合は,lepidic predominant adenocarcinomaと診断し,上皮内腺癌が疑われるとコメントをする.
微少浸潤性腺癌 Minimally invasive adenocarcinoma (MIA)


腫瘍径が3cm以下で,lepidicパターンが優位で,浸潤径が0.5cm以下の腺癌を微少浸潤性腺癌とする.
浸潤とは?
Lepidicパターンが優位でも,腫瘍径が3cmを超える場合や,浸潤径が0.5cmを超える場合は,lepidic predominant adenocarcinomaと診断する.
浸潤性腺癌 Invasive adenocarcinoma
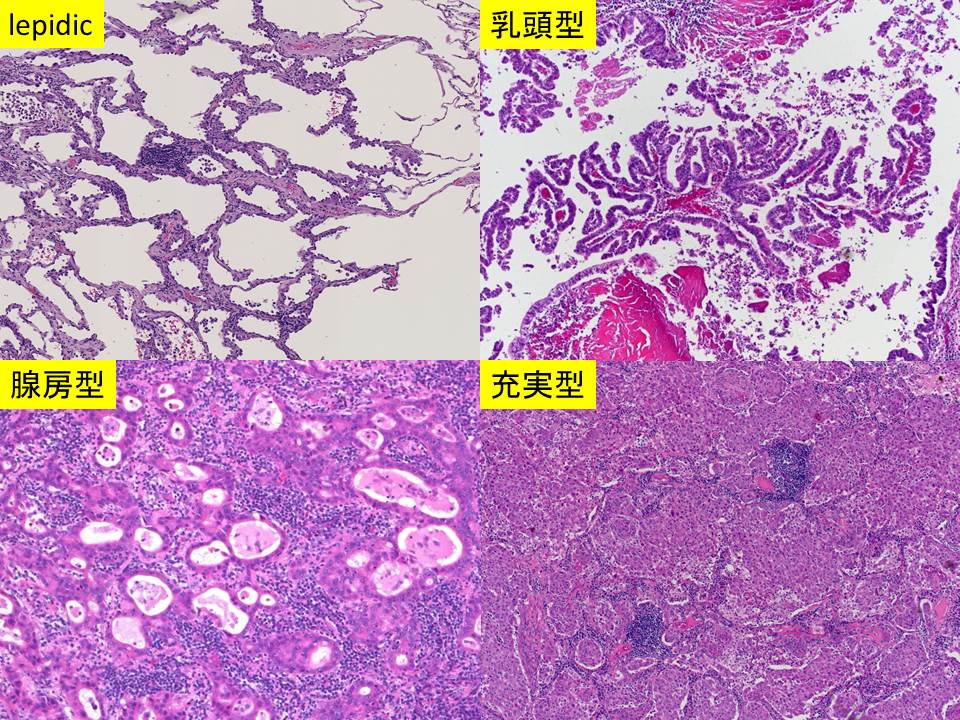
IASLC/ATS/ERS新分類では,混合型腺癌(adenocarcinoma mixed subtype)を用いず,これに相当するものとして,浸潤性腺癌を用いる.腫瘍内に存在するパターン(lepidic,腺房型,乳頭型,微小乳頭型,粘液産生充実型)の占める割合を5%きざみで記録する.浸潤性腺癌は,優位な組織パターンによりlepidic adenocarcinoma,腺房型(acinar adenocarcinom),乳頭型(papillary adenocarcinoma),微小乳頭型(micropapillary adenocarcinoma),充実型(solid adenocarcinoma)に亜分類する.従来混合型腺癌に分類されていた粘液非産生性BAC優位の腺癌は,lepidic predominant adenocarcinoma (LPA)に分類する.
早期腺癌において微小乳頭型は予後が不良である.
特殊型
特殊型として,浸潤性粘液腺癌(従来の粘液産生性BAC)invasive mucinous adenocarcinoma,コロイド腺癌colloid adenocarcinoma,胎児型腺癌fetal adenocarcinoma(低異型度,高異型度),腸型腺癌enteric adenocarcinomaをあげている.
浸潤性粘液腺癌 Invasive mucinous adenocarcinoma

従来の粘液産生性(mucinous) BACは,臨床的にも放射線画像的にも従来の粘液非産生性(nonmucinous) BACとは異なる.したがって,この腫瘍は以前のnonmucinous BACとは別に分類し,lepidic growthと浸潤径により粘液産生性上皮内腺癌mucinous AIS, 粘液産生性微少浸潤性腺癌mucinous MIA, 浸潤性粘液腺癌invasive mucinous adenocarcinomaに分類する.
粘液産生性上皮内腺癌 Mucinous AIS
Mucinous AISは,腫瘍径が3cm以下で,浸潤がない.
粘液産生性微少浸潤性腺癌 Mucinous MIA
Mucinous MIAは腫瘍径が3cm以下で,浸潤径が0.5cm以下である.
浸潤性粘液腺癌 Invasive mucinous adenocarcinoma
浸潤性粘液腺癌は多発性であり,他の肺葉,対側肺にも病変を認めることが多い.周囲の肺胞に腫瘍が散布状に広がるため腫瘍の境界は明瞭ではない.腫瘍細胞は杯細胞様あるいは円柱状である.腫瘍細胞の異型性は通常,軽度である.浸潤性粘液腺癌もlepidicパターン,腺房型,乳頭型,微小乳頭型,充実型の各パターンを示す.粘液を産生しても,杯細胞様あるいは高円柱状ではない場合は,浸潤性粘液腺癌とはしない.
粘液産生性・非産生性混合型腺癌 Mixed invasive mucinous and non-mucinous adenocarcinoma
粘液産生性腺癌と粘液非産生性腺癌が混合することがあり,それぞれが10%以上を占める.
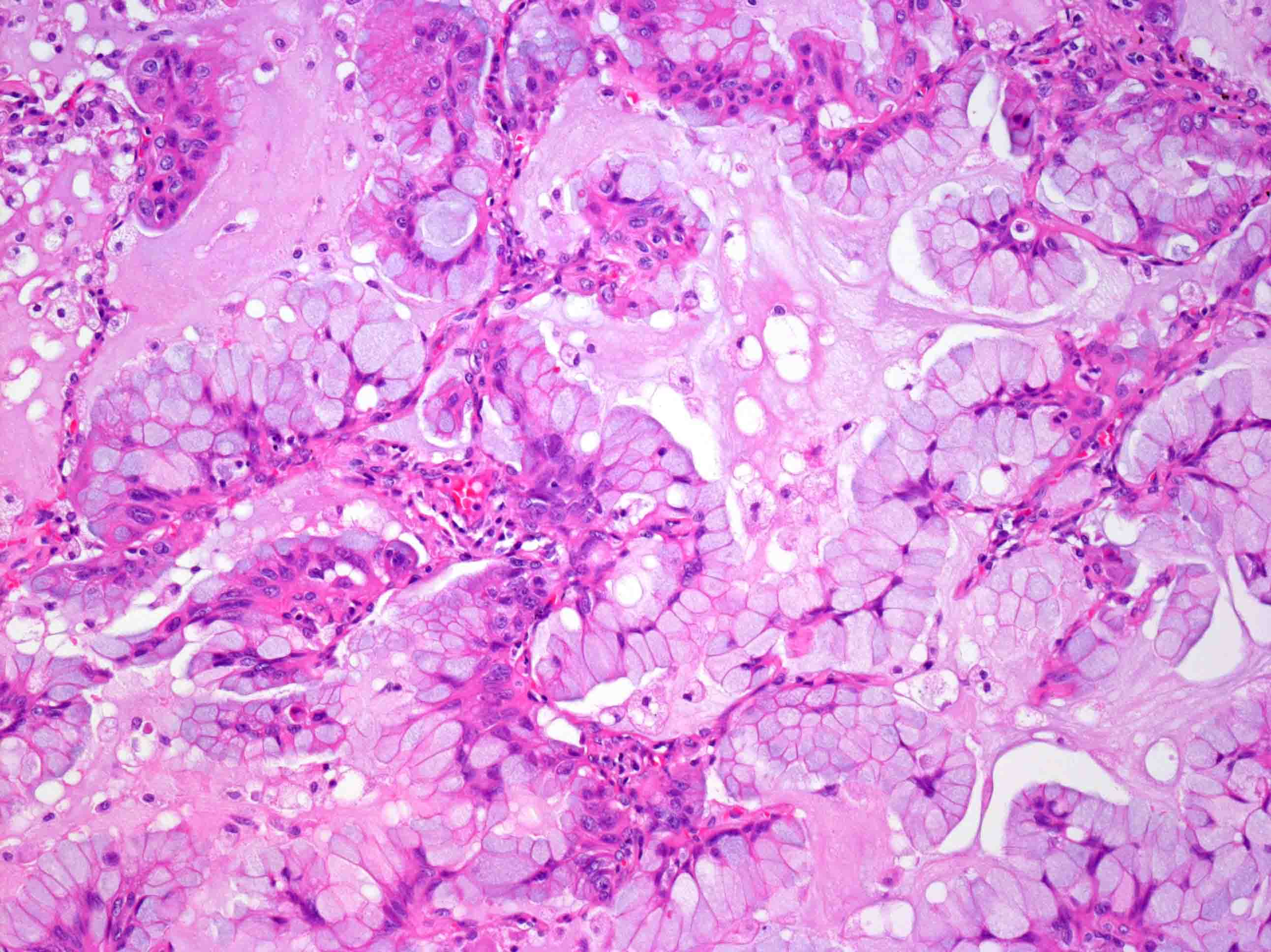
コロイド腺癌 Colloid adenocarcinoma


コロイド腺癌は,細胞外に多量の粘液を認め,肺胞腔が拡張し,肺胞壁が破壊されている.腫瘍細胞は粘液の中に浮遊している.1999年および2004年のWHO分類に記載がある粘液嚢胞腺癌mucinous cystadenocarcinomaは極めてまれであり,コロイド腺癌と同じスペクトラムにあると考えられるため,コロイド腺癌に分類する.
胎児型腺癌 Fetal adenocarcinoma


胎児型腺癌は,グリコーゲンに富む無線毛細胞が腺腔を形成し,胎児の肺に類似している.核上,核下空胞を認める.低異型度胎児型腺癌は,moruleとよばれる球状集塊を認め,核にoptically clear nucleusとよばれるすりガラス状変化を伴う.この核はビオチンに富む[3].βカテニン遺伝子の異常により発生し,免疫染色でβカテニンは,腫瘍細胞の核および細胞質が陽性になる[4, 5].高異型度胎児型腺癌はβカテニン遺伝子の異常は認めず,免疫染色でβカテニンは腫瘍細胞の細胞膜が陽性になる.前者は後者よりも若年者に発生し,予後が良好である.
腸型腺癌 Enteric adenocarcinoma


腸型腺癌は腸上皮への分化を伴う細胞が腫瘍の50%以上を占めるものをいう.大腸癌の肺転移とは異なり,組織像が多彩で,通常の肺腺癌の組織像もみられる.腫瘍細胞は高円柱状で,核の偽重層化を認め,腺腔形成,乳頭状増殖を示し,篩状配列を示すこともある.免疫染色は腸上皮への分化を示すCDX-2, CK20, MUC2などが陽性になる.約半数の症例は,CK7, TTF-1も陽性になるので,肺原発か大腸癌の転移かの鑑別に役立つ.
印環細胞癌signet ring adenocarcinoma,淡明細胞腺癌はclear cell adenocarcinomaは他の組織パターンに合併してみられる細胞学的変化である.これらが存在する場合は,その組織パターンの範囲を記録するべきであるが,充実型との間に臨床的な差異がみられないため,IASLC/ATS/ERS新分類の組織分類からは削除された.しかし,ALK遺伝子の再構成が存在する肺癌には印環細胞癌を含む頻度が高く[6],ALK遺伝子の再構成を伴う腺癌はALK tyrosine kinase inhibitor (TKI)であるcrizotinibが奏功することが報告されている[7, 8].
印環細胞癌の像を示す腺癌 solid adenocarcinoma with signet ring cell feature
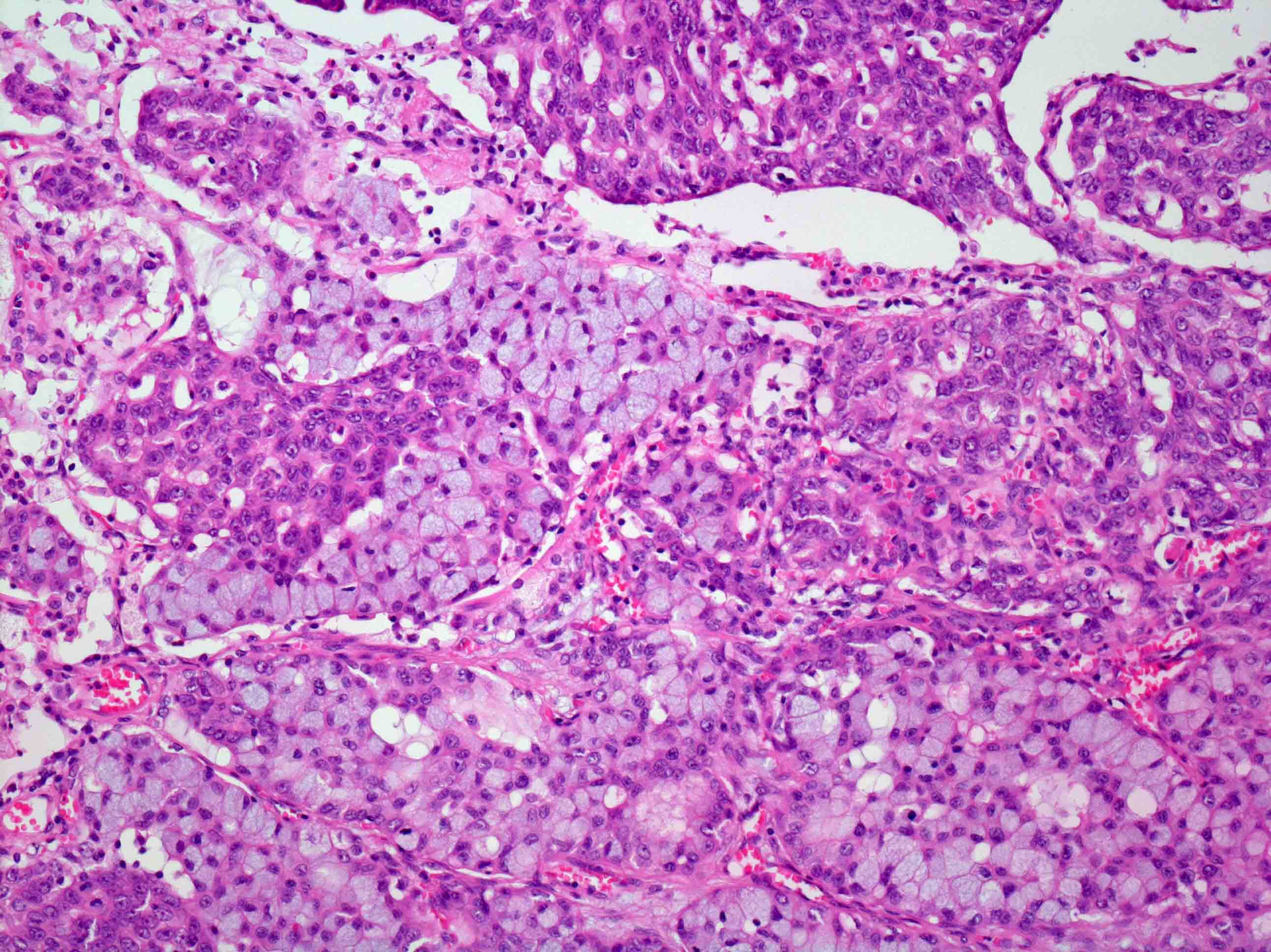
左図:印環細胞癌の像を示す癌細胞が充実性に増殖をしている.
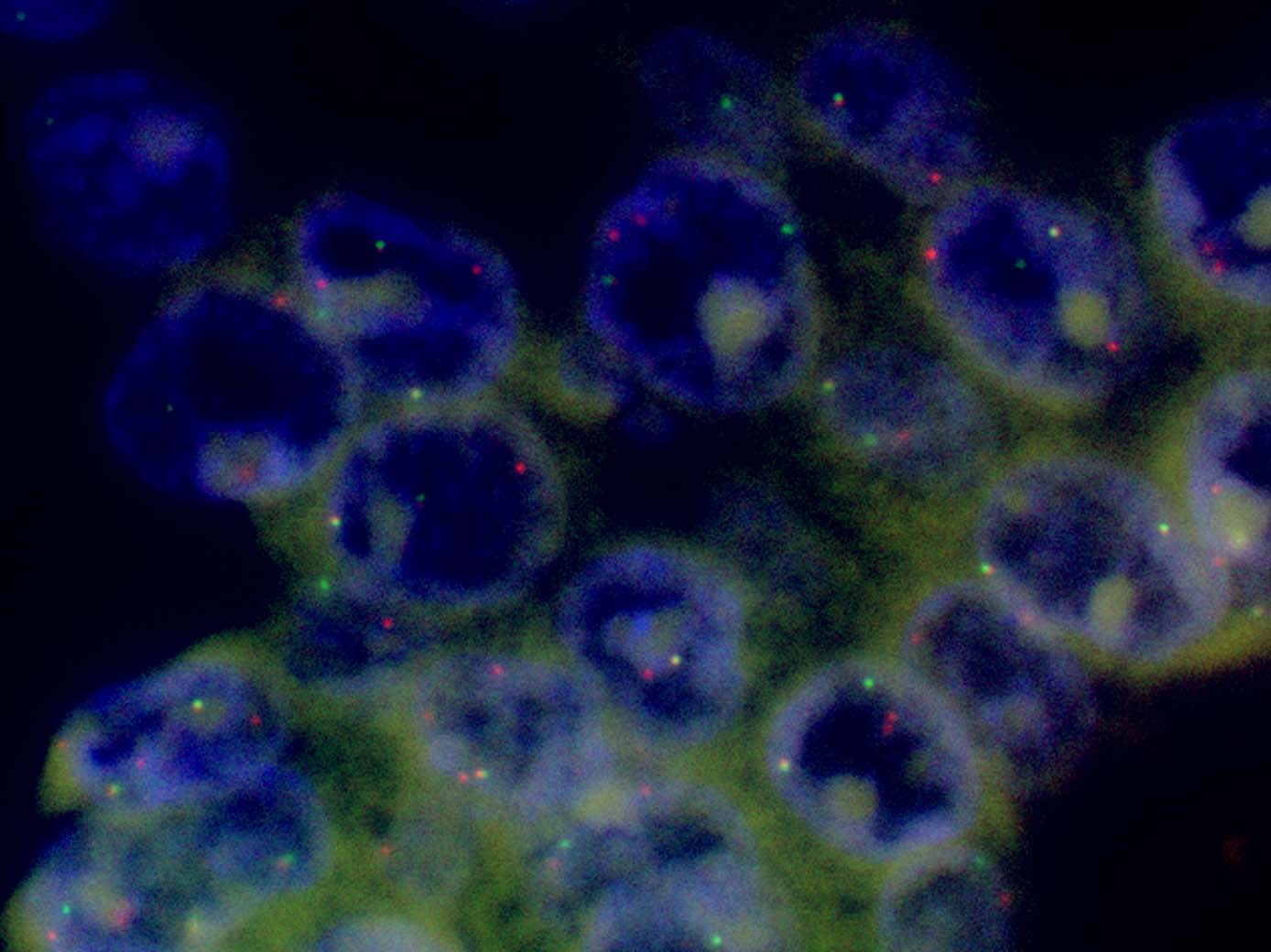
右図:FISHによりALK遺伝子が転座をおこしていることがわかる.
Spread through air spaces (STAS)

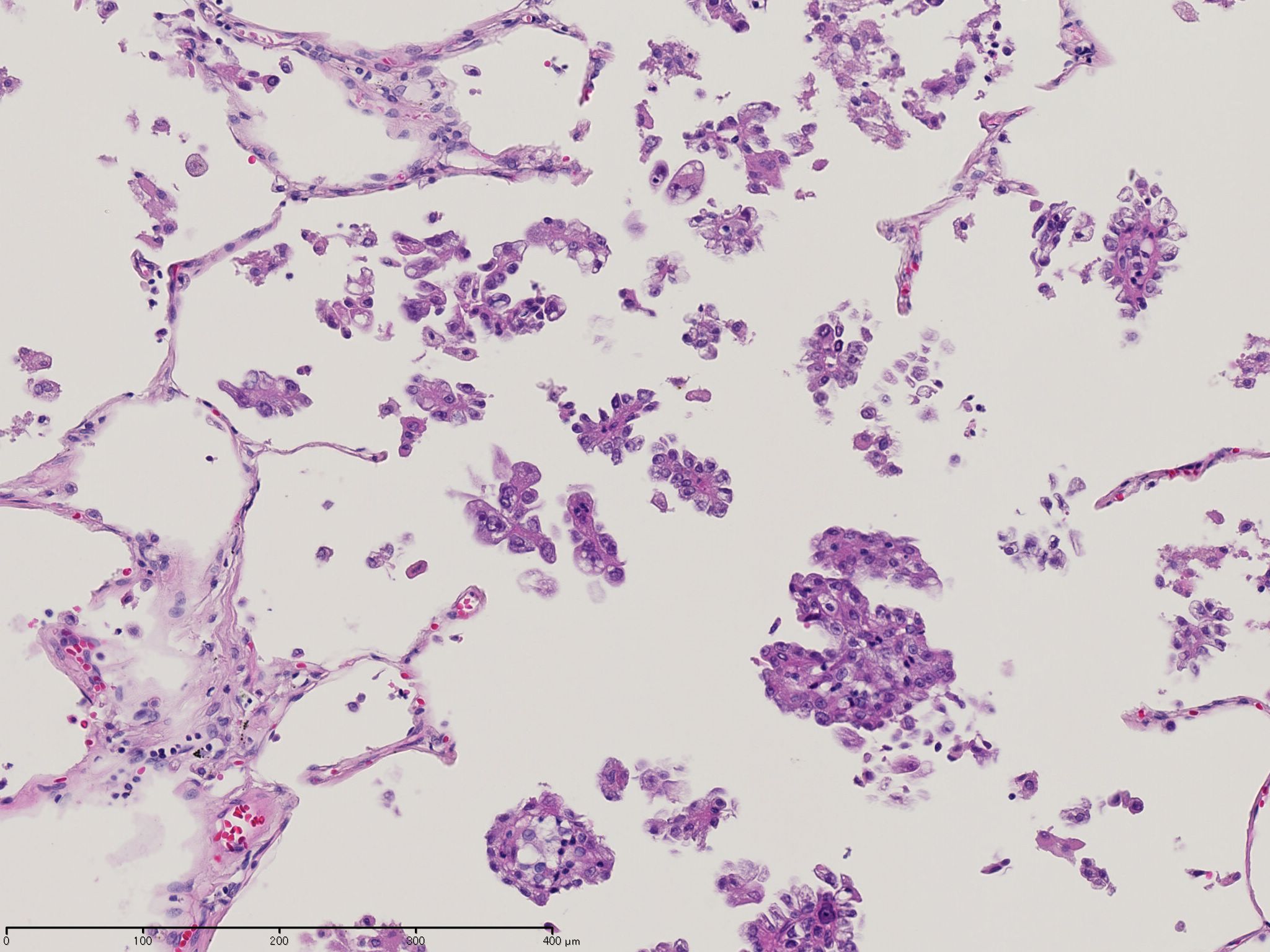
腫瘍の辺縁から周囲の肺胞腔内に微小乳頭状のクラスター,充実性胞巣,孤立性腫瘍細胞を認めることがある.病期Iの小型の腺癌に対して部分切除をした場合に,この所見があると再発の可能性が高い.STASは腫瘍の進展様式であり,腺癌のパターンとしてその占める割合を測定しない.また,腫瘍径にも入れない.
腺癌の組織亜型と遺伝子異常
腺癌の遺伝子異常と組織型にはある程度関係がある.KRAS突然変異は浸潤性粘液腺癌で頻度が高く[2, 14],また,乳頭型,充実型,中分化から低分化の腺癌で頻度が高い[14-17].EGFR突然変異は粘液非産生性lepidicパターン,非充実型で頻度が高く[2, 16, 17],中分化から高分化の腺癌で頻度が高い[14].ALK遺伝子の再構成は印環細胞癌を含む肺腺癌の頻度が高く[6],組織亜型は,乳頭型,粘液腺癌で頻度が高い[16].EGFR遺伝子, ALK遺伝子の異常を示す肺癌の核異型度は,KRAS遺伝子の異常を示す肺癌の核異型度よりも低い[16].
引用文献
1) World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. In: Travis W, Brambilla E, Muller-Hermelink H, Harris C, editors. Lyon: IARC Press, 2004:10-124.
2) Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol 2011;6:244-285.
3) Nakatani Y, Kitamura H, Inayama Y, Ogawa N. Pulmonary endodermal tumor resembling fetal lung. The optically clear nucleus is rich in biotin. Am J Surg Pathol 1994;18:637-642.
4) Nakatani Y, Masudo K, Miyagi Y, Inayama Y, Kawano N, Tanaka Y, et al. Aberrant nuclear localization and gene mutation of beta-catenin in low-grade adenocarcinoma of fetal lung type: up-regulation of the Wnt signaling pathway may be a common denominator for the development of tumors that form morules. Mod Pathol 2002;15:617-624.
5) Sekine S, Shibata T, Matsuno Y, Maeshima A, Ishii G, Sakamoto M, et al. Beta-catenin mutations in pulmonary blastomas: association with morule formation. J Pathol 2003;200:214-221.
6) Rodig SJ, Mino-Kenudson M, Dacic S, Yeap BY, Shaw A, Barletta JA, et al. Unique clinicopathologic features characterize ALK-rearranged lung adenocarcinoma in the western population. Clin Cancer Res 2009;15:5216-5223.
7) Kwak EL, Bang YJ, Camidge DR, Shaw AT, Solomon B, Maki RG, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med 2010;363:1693-1703.
8) Shaw AT, Yeap BY, Solomon BJ, Riely GJ, Gainor J, Engelman JA, et al. Effect of crizotinib on overall survival in patients with advanced non-small-cell lung cancer harbouring ALK gene rearrangement: a retrospective analysis. Lancet Oncol 2011;12:1004-1012.
9) Yoshizawa A, Motoi N, Riely GJ, Sima CS, Gerald WL, Kris MG, et al. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod Pathol 2011;24:653-664.
10) Yoshizawa A, Sumiyoshi S, Sonobe M, Kobayashi M, Fujimoto M, Kawakami F, et al. Validation of the IASLC/ATS/ERS lung adenocarcinoma classification for prognosis and association with EGFR and KRAS gene mutations: analysis of 440 Japanese patients. J Thorac Oncol 2013;8:52-61.
11) Warth A, Muley T, Meister M, Stenzinger A, Thomas M, Schirmacher P, et al. The novel histologic International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification system of lung adenocarcinoma is a stage-independent predictor of survival. J Clin Oncol 2012;30:1438-1446.
12) Thunnissen E, Beasley MB, Borczuk AC, Brambilla E, Chirieac LR, Dacic S, et al. Reproducibility of histopathological subtypes and invasion in pulmonary adenocarcinoma. An international interobserver study. Mod Pathol 2012;25:1574-1583.
13) Warth A, Cortis J, Fink L, Fisseler-Eckhoff A, Geddert H, Hager T, et al. Training increases concordance in classifying pulmonary adenocarcinomas according to the novel IASLC/ATS/ERS classification. Virchows Arch 2012;461:185-193.
14) Dacic S, Shuai Y, Yousem S, Ohori P, Nikiforova M. Clinicopathological predictors of EGFR/KRAS mutational status in primary lung adenocarcinomas. Mod Pathol 2010;23:159-168.
15) Rodenhuis S, Slebos RJ. Clinical significance of ras oncogene activation in human lung cancer. Cancer Res 1992;52:2665s-2669s.
16) Motoi N, Sato S, Saito Y, Ninomiya H, Takeuchi K, Ishikawa Y. Correlation between morphologic phenotype and genotype of lung adenocarcinoma based on a new IASLC/ATS/ERS classification with nuclear grading. Mod Pathol 2013;26:461A.
17) Ang DC, Zakowski MF, Ladanyi M, Moreira AL, Rekhtman N. Characteristic morphology and immunoprofile of lung adenocarcinoma with KRAS mutations: propensity for solid growth pattern and correlation with TTF-1 expression. Mod Pathol 2010;23:396A.
18) Bishop JA, Teruya-Feldstein J, Westra WH, Pelosi G, Travis WD, Rekhtman N. p40 (DeltaNp63) is superior to p63 for the diagnosis of pulmonary squamous cell carcinoma. Mod Pathol 2012;25:405-415.
19) Pelosi G, Fabbri A, Bianchi F, Maisonneuve P, Rossi G, Barbareschi M, et al. DeltaNp63 (p40) and thyroid transcription factor-1 immunoreactivity on small biopsies or cellblocks for typing non-small cell lung cancer: a novel two-hit, sparing-material approach. J Thorac Oncol 2012;7:281-290.
20) Churg A. The fine structure of large cell undifferentiated carcinoma of the lung. Evidence for its relation to squamous cell carcinomas and adenocarcinomas. Hum Pathol 1978;9:143-156.
21) Barbareschi M, Cantaloni C, Del Vescovo V, Cavazza A, Monica V, Carella R, et al. Heterogeneity of large cell carcinoma of the lung: an immunophenotypic and miRNA-based analysis. Am J Clin Pathol 2011;136:773-782.
22) Rekhtman N, Tafe LJ, Chaft JE, Wang L, Arcila ME, Colanta A, et al. Distinct profile of driver mutations and clinical features in immunomarker-defined subsets of pulmonary large-cell carcinoma. Mod Pathol 2013;26:511-522.